The idea — to take and cut a lens in a transparent cornea — is not new. At first it was done manually, with a scalpel directly on the surface (difficult and very rough, with a sea of side effects). The first laser was used in 1979, then it was a pulsed infrared emitter with an effective pulse length of 4 nanoseconds.
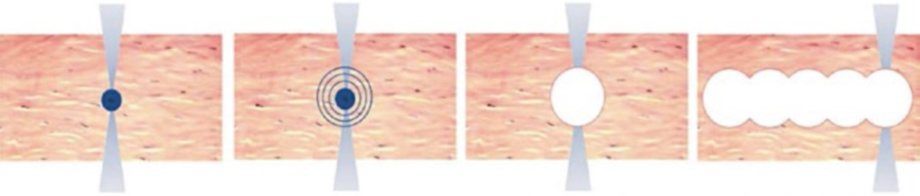
Step 1: creating a plasma bubble, in fact — a microburst. Step 2: expansion of the shock and heat waves. Step 3: cavitation bubble (plasma expansion). Step 4: the formation of a parallel slice at the expense of several adjacent laser focus points.
The main effect, which today after all the evolution of technology can be achieved with a laser, is that its cone can be focused in a sufficiently small area at a distance from the lens. If this focusing area is inside the cornea of the eye (even if it is transparent), then a microexplosion will actually occur, the resulting plasma bubbles will create a gap in the tissue.
Тoday, one “microexplosion” lasts not 4 nanoseconds, but 10,000 times faster.
The duration of the “microexplosion” depends on the operating frequency of the femtolaser (this is why it is called “femto”, because the pulses are femtosecond). The surface of the cornea itself remains intact: the incisions go straight through the thickness of the transparent layer.
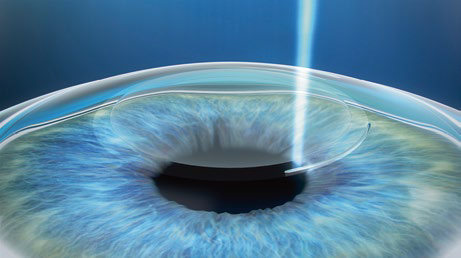
A frame from the ReLEx telemetry — a lens-lenticular lens is cut out from about 4 million laser pulses inside the eye, it is removed through a 2.5-mm incision at the edge, touching the surface. Today let's talk about the laser that does it.
In the 1980s, a bright idea appeared not only to use the capabilities of the laser itself, but also to fasten to it the carriage from the CNC machine to provide automatic control. In 2001, the first femtolaser under CNC was tested for accurate medical interventions suitable for working on human eyes (before that it had other medical uses and then was tested unchanged for about 6 years in rabbits and pigs — this is a normal procedure).
The first type of procedure is a femtolaser wide incision around the circumference of the cornea to form a kind of “lid” (flap). Then the correction is made, in fact, by evaporation of the tissue by an ex-world laser. This is what was the cutting edge of medicine about 5 years ago. You know the obvious advantages of laser vision correction, and if you haven’t done it yet because of fears of side effects, congratulations, you were right and waited.
The main problem of the method, simplifying, is poor healing.
The first difficulty is that the cornea rests on one thin flap at the edge — the “lid loop”. Considering the peculiarities of corneal tissue regeneration, it never “grows” back (this would mean closing the eye with connective tissue, that is, blocking the optic canal, the body does not do this). The problem is that an eye injury causes a waste of this layer, and often with extremely unpleasant consequences. In my practice, I came across with quite understandable reasons, such as a hard hit in an accident, hit with sports equipment to the head, blows in a fight, and much more prosaic, but incredibly worsening the patient's quality of life. For example, about five times there was a case in young mothers: «the child was sitting on his knees, playing, accidentally touching his eye with a finger.» Repeated operation to restore this «cover» is possible with fast handling,
The second feature is a violation of the innervation of the eye due to a sufficiently strong laser effect (wide deep cuts are required). Again, significantly simplifying, the top layer of the cornea of the eye successfully regenerates, and if we don’t transfer too much heat to it, then much can be done with it. However, we are worried about the next layer — the Bowman's membrane, which lies a little deeper. It does not regenerate under any circumstances, and any damage to the Bowman's membrane can be considered irreversible. In the case of a procedure with the formation of a flap (“cover”), for example, relatively modern LASIK, a wide and deep incision is made that touches this layer and transfers quite a lot of heat to it. Here is a schematic comparison of the methods:

Figure 1 — the usual location of the nerves, 2 — after the LASIK or FLEX procedure (where the flap cutout is required), 3 — after the ReLEx SMILE procedure, the dashed line shows the borders of the lenticules, the solid line shows the incision through which it is removed from the eye
That is, with any laser correction, some of the nerves will still suffer and will be cut off, and the Bowman's membrane will in any case be injured. The question is how serious it will be. The principal difference is 340 degrees of arc of a cut or only about 10 degrees of arc to remove lenticules. I remind you that we are worried not only by the physical incision itself, but also by the rather serious heating of eye tissue in the immediate vicinity of a laser beam evaporating corneal tissue. In theory, it would be possible to reduce heat by dividing the procedure into ten to twenty parts, but this, alas, is not yet possible; it will not be possible to keep the eye still on the pneumatic grip system for so long. But about this system and its work — in the next post.
Here is the SMILE (Small Incision Lenticule Extraction) method with one cut from the surface (there is also a version with two, but about the difference a bit later). For now — renders.
A first incision is made inside the cornea, forming the lower border of the lens:
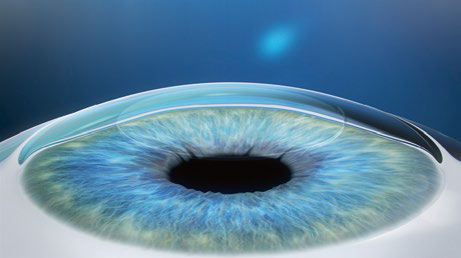
The second cut is slightly higher to form the upper border of the lens:
This is how it looks (schematic diagram, it does not convey the scale):
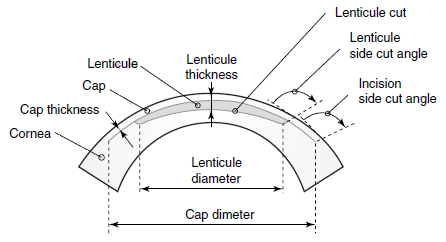
Here is the lentikula itself schematically:

Lenticle form for operation in a patient with myopia (-5 diopters) in real proportions. The diameter is 6 millimeters, the thickness at the edge is 15 micrometers, the edge is cut at a right angle.
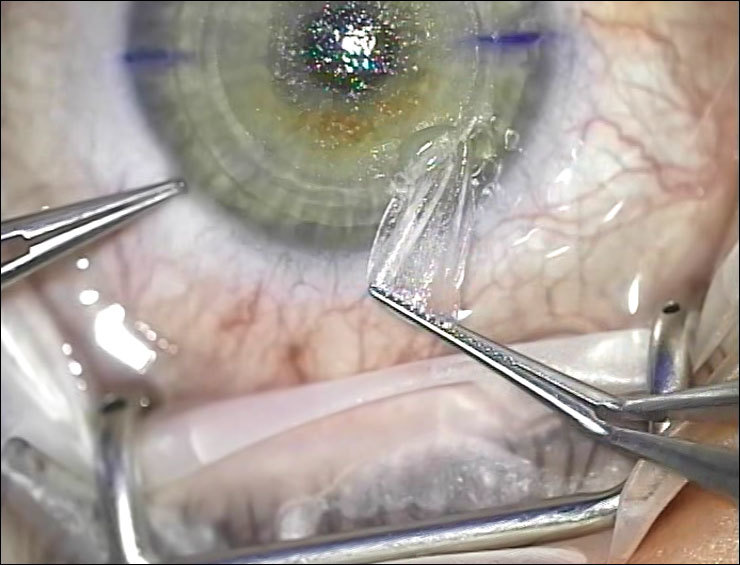
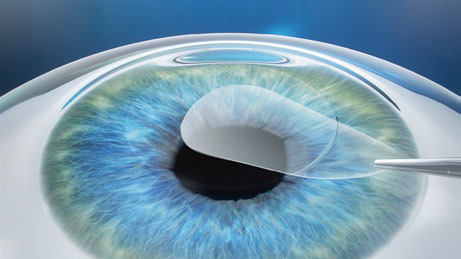
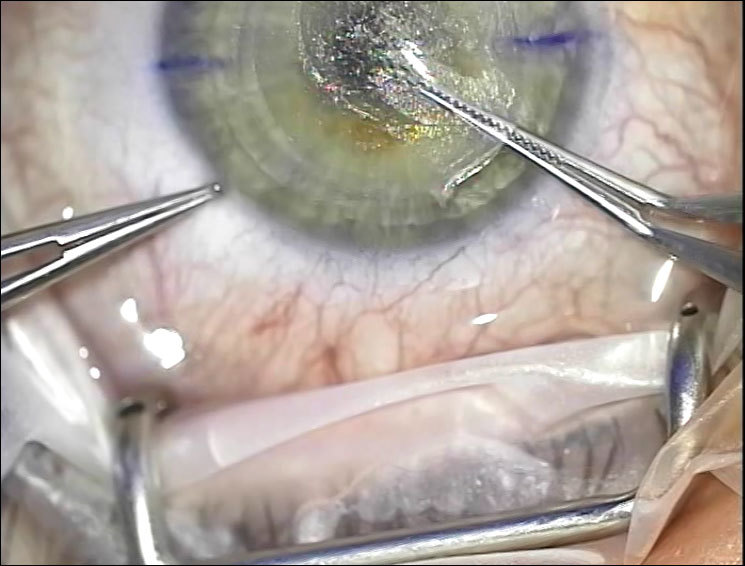
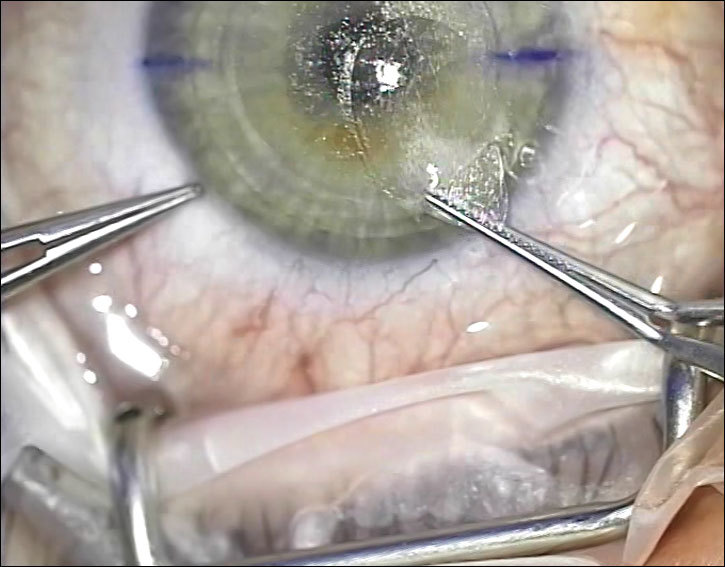
Then lenticular is separated with a blunt spatula and removed from the eye by the surgeon performing the operation (this is done with tweezers). Here, in fact, the difference between the render and the real operation:
n order to cut the lens on the surface of the eye, you need about a million micro-fractures, that is, about a million focus points at which plasma bubbles are created.
For an even cut you need from 10 thousand to 100 thousand focus points per square millimeter. In order to cut the inside of the cornea «lens» with a diameter of 7 millimeters (the most common case), you need about 4.3 million laser pulses. The primary effect is the creation of a plasma «ball», the secondary is the expansion of plasma and relatively safe tissue separation without significant damage. And this is on condition that they hit the target, by the way, which is not at all a fact due to the variable properties of the medium between the lens and the focus point, floating on the eye of fat clots and other interesting things.
Why do you need femtolaser? Because the smaller the impulse, the smaller the plasma bubble results in, and the smaller the cut thickness will be. But what else is more important at times, the less thermal energy goes to the eye. Here it should be noted that this increases the risk of various injuries caused by heat exposure. Most often this means problems with innervation, in the common people — «dry eye». Less often — a painful change in the shape of the cornea, which can not be removed (keratoconus).
In 2008, the optimal impact was calculated — this is the frequency from 500 KHz with the minimum energy per separate pulse.
That's all for today.
Illustrations from L. Mastropasqua and M. Nubile, Small Incision Lenticule Extraction (SMILE).
If interested, we are now working together with the author of technology, professor, doctor of honey. n Walter Sekundo, who has the longest experience on the planet in working with femtolasers for vision correction. It was he who developed the method of operation and many tools for it. You may be interested in:
Often, writing will not work, answering everything in fragments, too, will not work, so choose what the next post will be about.
Step 1: creating a plasma bubble, in fact — a microburst. Step 2: expansion of the shock and heat waves. Step 3: cavitation bubble (plasma expansion). Step 4: the formation of a parallel slice at the expense of several adjacent laser focus points.
The main effect, which today after all the evolution of technology can be achieved with a laser, is that its cone can be focused in a sufficiently small area at a distance from the lens. If this focusing area is inside the cornea of the eye (even if it is transparent), then a microexplosion will actually occur, the resulting plasma bubbles will create a gap in the tissue.
Тoday, one “microexplosion” lasts not 4 nanoseconds, but 10,000 times faster.
The duration of the “microexplosion” depends on the operating frequency of the femtolaser (this is why it is called “femto”, because the pulses are femtosecond). The surface of the cornea itself remains intact: the incisions go straight through the thickness of the transparent layer.
A frame from the ReLEx telemetry — a lens-lenticular lens is cut out from about 4 million laser pulses inside the eye, it is removed through a 2.5-mm incision at the edge, touching the surface. Today let's talk about the laser that does it.
What is the classic correction procedure (for example, LASIK)?
In the 1980s, a bright idea appeared not only to use the capabilities of the laser itself, but also to fasten to it the carriage from the CNC machine to provide automatic control. In 2001, the first femtolaser under CNC was tested for accurate medical interventions suitable for working on human eyes (before that it had other medical uses and then was tested unchanged for about 6 years in rabbits and pigs — this is a normal procedure).
The first type of procedure is a femtolaser wide incision around the circumference of the cornea to form a kind of “lid” (flap). Then the correction is made, in fact, by evaporation of the tissue by an ex-world laser. This is what was the cutting edge of medicine about 5 years ago. You know the obvious advantages of laser vision correction, and if you haven’t done it yet because of fears of side effects, congratulations, you were right and waited.
The main problem of the method, simplifying, is poor healing.
The first difficulty is that the cornea rests on one thin flap at the edge — the “lid loop”. Considering the peculiarities of corneal tissue regeneration, it never “grows” back (this would mean closing the eye with connective tissue, that is, blocking the optic canal, the body does not do this). The problem is that an eye injury causes a waste of this layer, and often with extremely unpleasant consequences. In my practice, I came across with quite understandable reasons, such as a hard hit in an accident, hit with sports equipment to the head, blows in a fight, and much more prosaic, but incredibly worsening the patient's quality of life. For example, about five times there was a case in young mothers: «the child was sitting on his knees, playing, accidentally touching his eye with a finger.» Repeated operation to restore this «cover» is possible with fast handling,
The second feature is a violation of the innervation of the eye due to a sufficiently strong laser effect (wide deep cuts are required). Again, significantly simplifying, the top layer of the cornea of the eye successfully regenerates, and if we don’t transfer too much heat to it, then much can be done with it. However, we are worried about the next layer — the Bowman's membrane, which lies a little deeper. It does not regenerate under any circumstances, and any damage to the Bowman's membrane can be considered irreversible. In the case of a procedure with the formation of a flap (“cover”), for example, relatively modern LASIK, a wide and deep incision is made that touches this layer and transfers quite a lot of heat to it. Here is a schematic comparison of the methods:
Figure 1 — the usual location of the nerves, 2 — after the LASIK or FLEX procedure (where the flap cutout is required), 3 — after the ReLEx SMILE procedure, the dashed line shows the borders of the lenticules, the solid line shows the incision through which it is removed from the eye
That is, with any laser correction, some of the nerves will still suffer and will be cut off, and the Bowman's membrane will in any case be injured. The question is how serious it will be. The principal difference is 340 degrees of arc of a cut or only about 10 degrees of arc to remove lenticules. I remind you that we are worried not only by the physical incision itself, but also by the rather serious heating of eye tissue in the immediate vicinity of a laser beam evaporating corneal tissue. In theory, it would be possible to reduce heat by dividing the procedure into ten to twenty parts, but this, alas, is not yet possible; it will not be possible to keep the eye still on the pneumatic grip system for so long. But about this system and its work — in the next post.
How ReLEx SMILE Works
Here is the SMILE (Small Incision Lenticule Extraction) method with one cut from the surface (there is also a version with two, but about the difference a bit later). For now — renders.
A first incision is made inside the cornea, forming the lower border of the lens:
The second cut is slightly higher to form the upper border of the lens:
This is how it looks (schematic diagram, it does not convey the scale):
Here is the lentikula itself schematically:
Lenticle form for operation in a patient with myopia (-5 diopters) in real proportions. The diameter is 6 millimeters, the thickness at the edge is 15 micrometers, the edge is cut at a right angle.
Then lenticular is separated with a blunt spatula and removed from the eye by the surgeon performing the operation (this is done with tweezers). Here, in fact, the difference between the render and the real operation:
How does such a laser work?
n order to cut the lens on the surface of the eye, you need about a million micro-fractures, that is, about a million focus points at which plasma bubbles are created.
For an even cut you need from 10 thousand to 100 thousand focus points per square millimeter. In order to cut the inside of the cornea «lens» with a diameter of 7 millimeters (the most common case), you need about 4.3 million laser pulses. The primary effect is the creation of a plasma «ball», the secondary is the expansion of plasma and relatively safe tissue separation without significant damage. And this is on condition that they hit the target, by the way, which is not at all a fact due to the variable properties of the medium between the lens and the focus point, floating on the eye of fat clots and other interesting things.
Why do you need femtolaser? Because the smaller the impulse, the smaller the plasma bubble results in, and the smaller the cut thickness will be. But what else is more important at times, the less thermal energy goes to the eye. Here it should be noted that this increases the risk of various injuries caused by heat exposure. Most often this means problems with innervation, in the common people — «dry eye». Less often — a painful change in the shape of the cornea, which can not be removed (keratoconus).
In 2008, the optimal impact was calculated — this is the frequency from 500 KHz with the minimum energy per separate pulse.
That's all for today.
Illustrations from L. Mastropasqua and M. Nubile, Small Incision Lenticule Extraction (SMILE).
If interested, we are now working together with the author of technology, professor, doctor of honey. n Walter Sekundo, who has the longest experience on the planet in working with femtolasers for vision correction. It was he who developed the method of operation and many tools for it. You may be interested in:
- How the eye restraint system is designed during the operation and how the shape of the lenticule lens is created, why it turns out exactly and what depends on you, and what depends on the CNC and the skills of the surgeon. Well, why in fact the cut is made even when the patient thinks that preparation is underway.
- How exactly the lenticular gets: how the tissues behave at the border of the incisions, why it is necessary to separate them mechanically with a spatula, how such a spatula is arranged and how the eye wash is performed after the operation.
- What exactly are the types of operations for vision correction and what features, indications, pros and cons of each.
- A selection of years of clinical research: from how much the eye pressure rises when exposed to a laser, to what is more dangerous — an unhealed flap or 20 years of wearing contact lenses. With comments and explanations in human language.
- Well, for sweetness, we are now trying to coordinate with the German clinic SMILEEYES a publication for training purposes of full telemetry with human surgery. It looks really scary and can scare away almost any sensitive nature, believe me, but it is extremely interesting.
Often, writing will not work, answering everything in fragments, too, will not work, so choose what the next post will be about.

a-tk
Please remove this picture from article preview, it's so nasty.
Flagman
There isn’t much beautiful in medicine :) And in general this is a key illustration to the article
Bringoff
It should be on the main feed. Not all people are ready to see something on their feed even without opening the article.
Bringoff
Hm. Looks like my comment is missing a couple of words I definitely typed. This is what I've tried to say:
marsermd
Agreed. Surgical operations shouldn't be directly visible in the main feed.